Scottish Welfare Fund news - January 2024
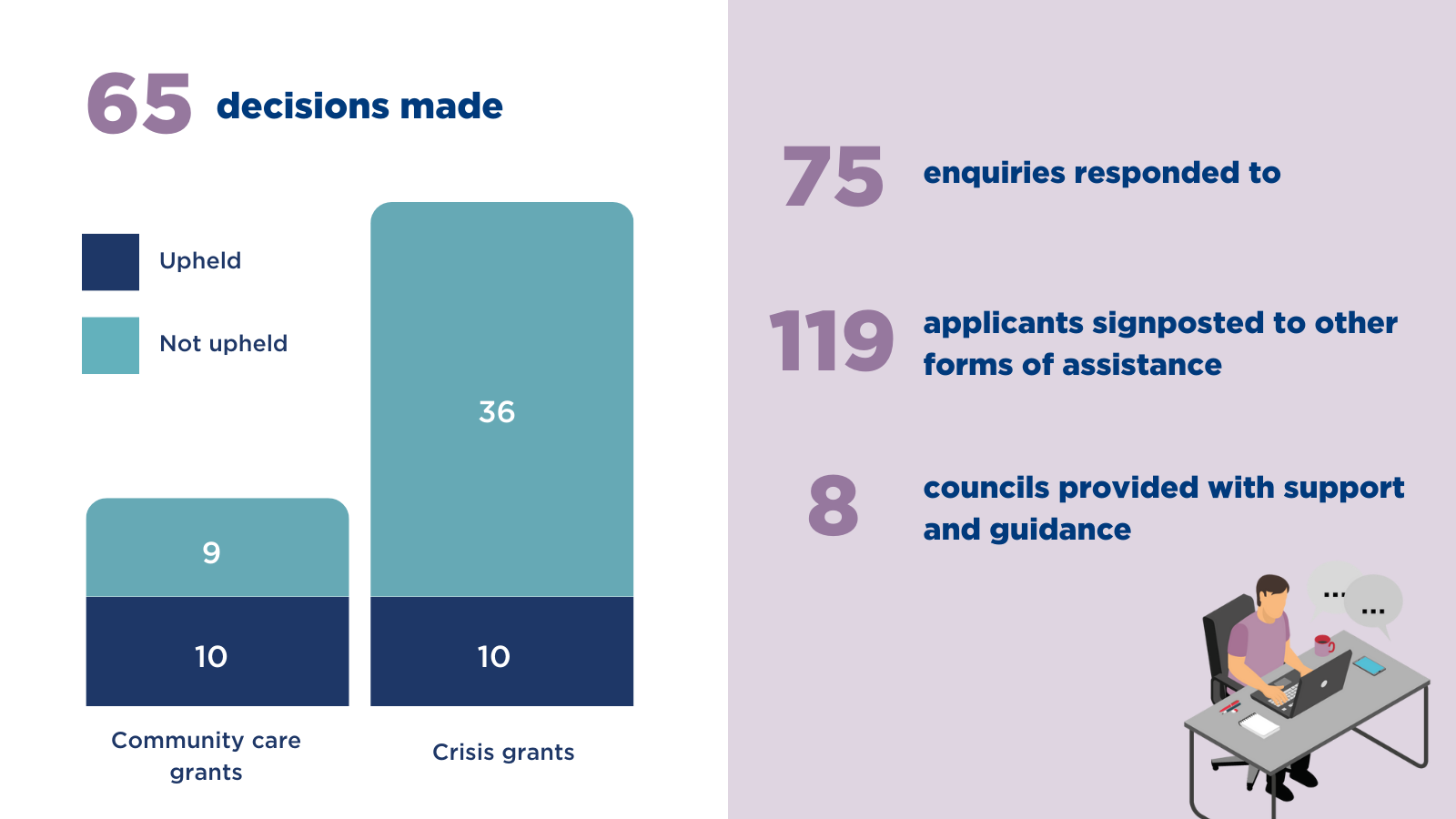
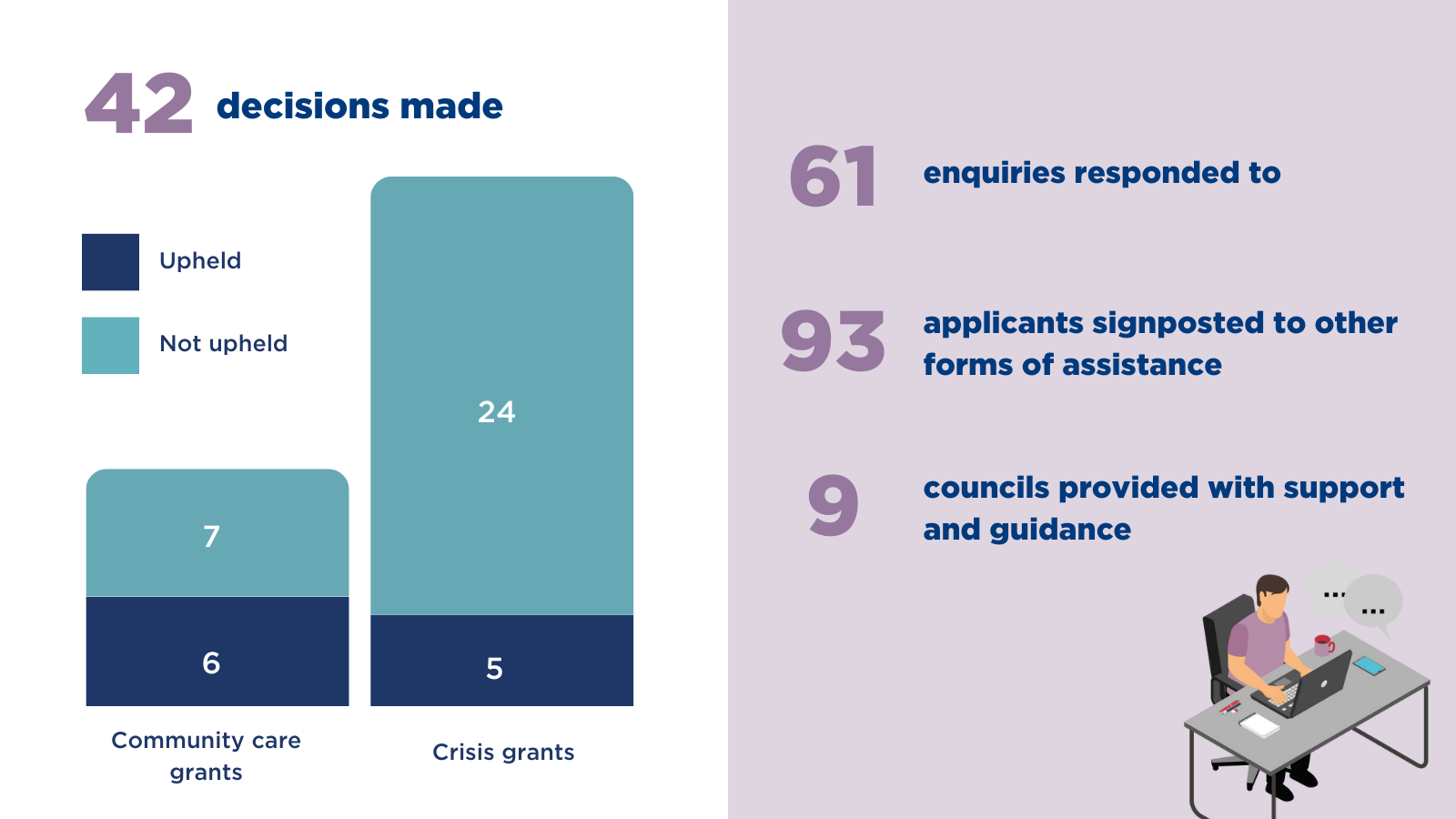
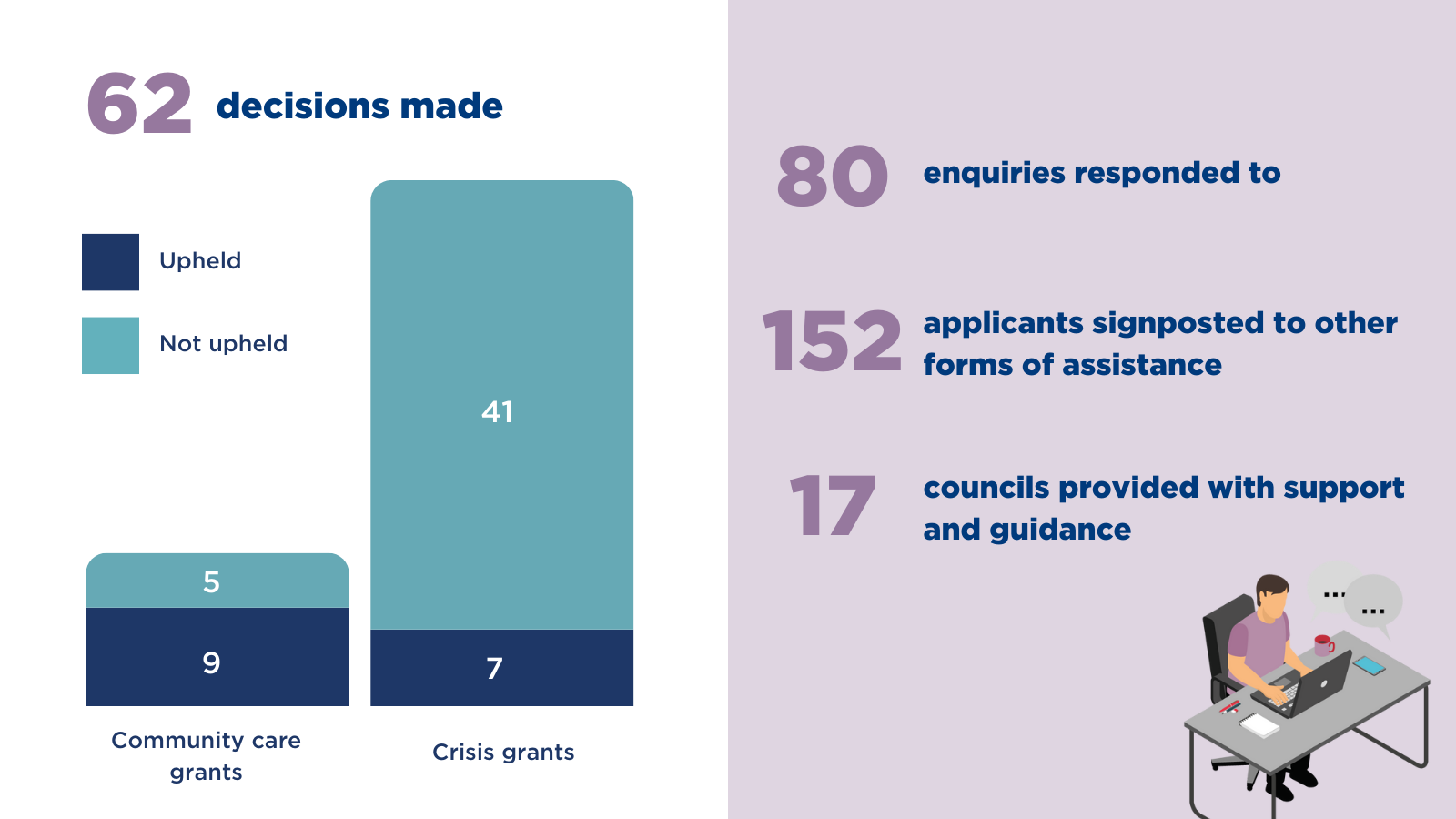
Last month we:
Last month we:
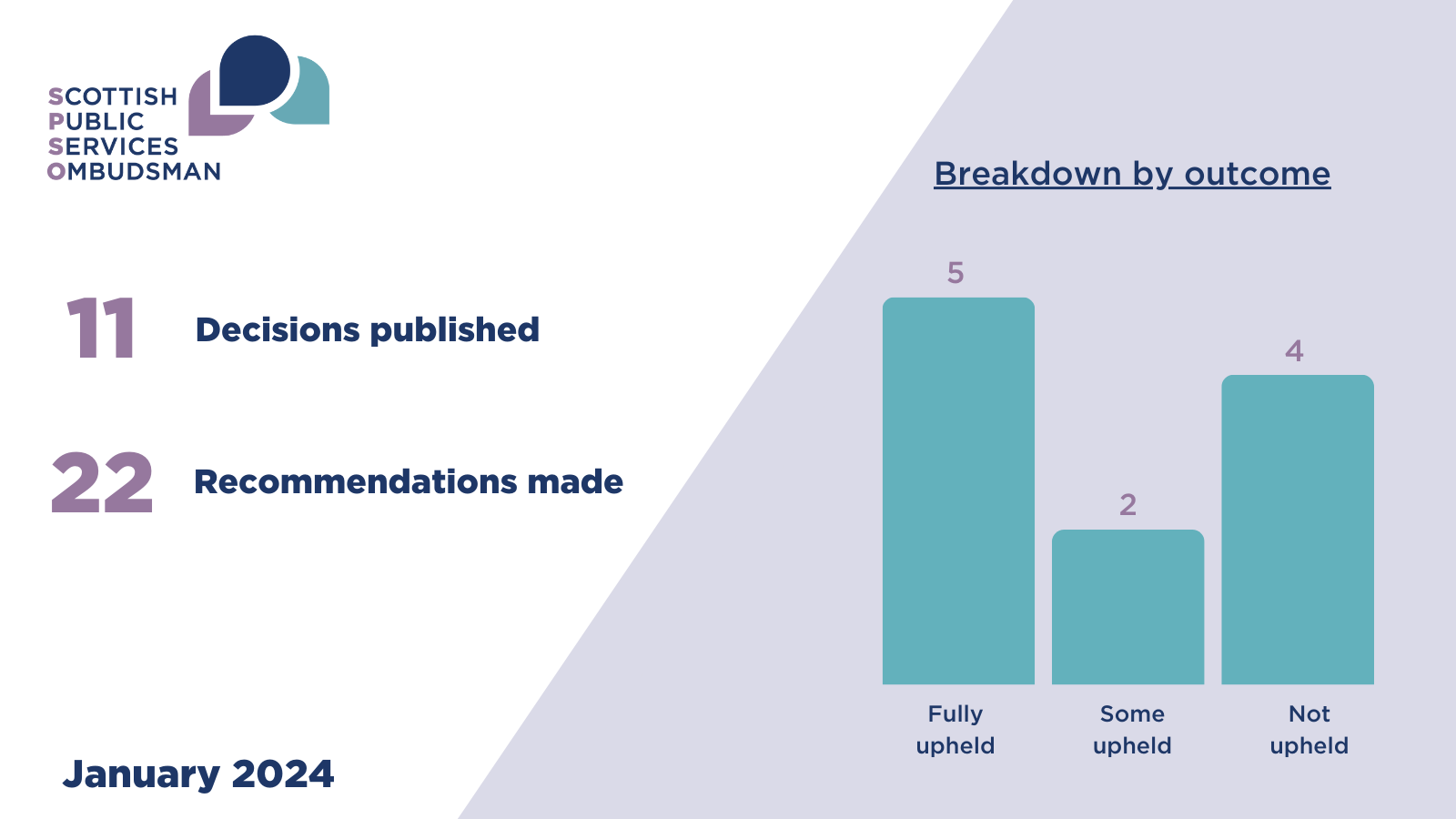
In this month’s edition of the Ombudsman’s findings, we highlight the importance of having robust systems and polices in place to ensure efficient and uninterrupted service delivery.

Our SPSO Conference 2023: Supporting Good Complaints Handling in a Changing World took place this year on Thursday 16 November 2023 at Murrayfield Stadium, Edinburgh.
Please note that this invitation to tender is now closed.
We are inviting tenders for the provision of soft phone telephony services. The successful contracts from this invitation to tender will:
The complainant (C) complained to my office about the care and treatment they received from Fife NHS Board (the Board) between April and May 2021. C received Dalteparin injections, a heparin-based treatment, from the Board’s outpatient Deep Vein Thrombosis (DVT) clinic for a superficial vein thrombophlebitis (SVT: inflammation of a vein near the surface of the skin). Around nine days after commencing the injections C reported to the clinic new onset of symptoms of weakness, numbness and difficulty moving their leg. C was admitted to hospital where they received investigations to rule out either peripheral nerve entrapment or a stroke. C’s symptoms continued to worsen including new onset of severe leg pain, and it was later confirmed that C had developed limb ischaemia (inadequate blood supply due to blockage of the blood vessels) due to Heparin Induced Thrombocytopenia (HIT), a serious complication associated with heparin-based products. Although C was transferred to another health board for emergency vascular surgery which saved their leg, they have been left with permanent nerve damage and suffer from chronic pain and reduced mobility.
C complained the delay in treating them for HIT resulted in the permanent harm caused to their leg, and their outcome would have been better had the condition been diagnosed and treated earlier. C also complained that the Board’s handling of their complaint had been unreasonable.
The Board said that C’s presentation of limb ischaemia was unusual, alongside an unusual but not unrecognised, side effect of heparin injections. Ruling out a stroke or spinal problem was the clinical priority. There was a missed opportunity to review C at the DVT clinic in light of the blood tests taken, and there was a failure to consider HIT earlier, timeous screening of which could have prompted an earlier prescription of a different anticoagulant drug to treat or prevent a blood clot. C complained to SPSO about this episode of care and the Board’s handling of their complaint, which they said had failed to recognise the harm caused to them by this incident. When my office contacted the Board about C’s complaint, the Board advised that a decision had been taken to undertake a Local Adverse Event Review (LAER). The complaint was closed by my office as it was considered the outcome of the LAER may resolve C’s remaining concerns. C contacted my office again some months later as they were yet to receive a copy of the LAER report and as the Board were unable to commit to a timescale for its completion. I made enquiries of the Board about the LAER and decided to investigate. The Board subsequently issued the LAER report, 11 months after the decision was made to commence the review process.
I sought independent advice from a Consultant Haematologist (the Adviser). The Adviser told me HIT is an infrequent rather than unusual complication of heparin injections and all patients receiving this treatment should be routinely monitored for this. The DVT clinic appointments were a key opportunity to manage C’s condition before harm had happened, particularly in light of the blood results which were available indicating that C’s platelet count had dropped. HIT is a very difficult condition to treat even when treatment is commenced immediately, however, had action been taken earlier, in their view, it may have significantly changed the outcome for C. It would be usual to treat for HIT urgently until proven otherwise, however, the investigations C received were focused on nerve entrapment or stroke. Had it been the case that C was suffering from a stroke, it would likely have occurred as a consequence of HIT, not as an independent occurrence. The link between HIT and the presence of a stroke had not been made and there was a failure to recognise the need to act on the likely diagnosis of HIT and start treatment straight away.
The Adviser noted the Board’s LAER report did not recognise that the haematology experts, both the DVT clinic and the on-call haematologist, failed to identify the significant change in C’s blood results which had occurred even before C first presented with leg symptoms. It was of significant concern that although junior and general medical staff correctly suspected HIT, they did not then receive appropriate specialist support and advice which meant C was not urgently treated for HIT as they should have been. The Adviser further said that they considered this incident to be a serious adverse event. As C was left with a permanent harm, the incident met the requirements for a category one Significant Adverse Event Review, as set out in guidance issued by Healthcare Improvement Scotland. The grounds on which a LAER or SAER would be commissioned were unclear in the Board’s policy, however, on balance it was unreasonable that this had not been investigated as a SAER.
In light of the evidence I have seen and the advice I have received and considered, I found that:
i. There was a failure to appropriately review and monitor C’s platelet count at the DVT clinic;
ii. There was a failure to appropriately assess and diagnose C for suspicion of HIT; provide appropriate haematology advice to medical staff and review and document C’s response to pain relief; and
iii. the Board’s handling of C’s complaint was unreasonable including their handling of the LAER
As such, I upheld C’s complaints.
What we are asking the Board to do for C:
| Complaint number |
What we found |
What the organisation should do |
What we need to see |
|---|---|---|---|
|
(a) |
i. appropriately review and monitor C’s platelet count at the DVT clinic. ii. appropriately assess and diagnose C for suspicion of HIT taking into account the timeframe of onset of symptoms or consider the working diagnosis of stroke as a likely manifestation of HIT. iii. provide appropriate haematology advice to medical staff iv. appropriately review and document C’s response to pain relief medication once their pain had escalated. |
Apologise to C for the failings identified in this report. The apology should meet the standards set out in the SPSO guidelines on apology available at www.spso.org.uk/information-leaflets. |
By: 24 January 2024
|
We are asking the board to improve the way they do things:
| Complaint number |
What we found |
What should change |
What we need to see |
|---|---|---|---|
|
(a) |
|
Bloods results should be appropriately reviewed and patients receiving heparin injections appropriately monitored. Patients should receive appropriate, timely review if any new onset symptoms are reported. |
By: 20 March 2024 |
| (a) |
i. appropriately assess and diagnose C for suspicion of HIT taking into account the timeframe of onset of symptoms or consider the working diagnosis of stroke as a likely manifestation of HIT. ii. provide appropriate haematology advice to medical staff. |
Patients presenting symptoms as in C’s case should be appropriately reviewed by general and speciality medical staff with reference to the timeframe of onset of symptoms and likely manifestations of HIT, such as stroke, with treatment commenced as appropriate. |
By: 20 March 2024
|
We are asking the board to improve their complaints handling:
| Complaint number |
What we found |
Outcome needed |
What we need to see |
|---|---|---|---|
|
(b) |
|
When an incident occurs that falls within the Duty of Candour legislation, the Board’s Duty of Candour processes should be activated without delay and the individual notified within the prescribed timescales. If there is a delay in notification a full explanation should be provided.
|
By: 20 March 2024
|
| (b) |
i. It failed to keep C informed of the process and the reasons for selecting a LAER, rather than SAER. ii. It failed to identify key learning from the circumstances of C’s complaint. iii. Significant (rather than a Local) adverse event review should have been held in line with relevant guidance. |
Local and Significant adverse event reviews should be reflective and learning processes that ensure failings are identified and any appropriate learning and improvement taken forward. The Board’s adverse event policy should be consistent with HIS guidance, and the type of investigation undertaken should be appropriate to the level of category identified. |
By: 17 April 2024 |
The Board told us they had already taken action to fix the problem. We will ask them for evidence that this has happened:
| Complaint number |
What we found |
Outcome needed |
What we need to see |
|---|---|---|---|
|
(b) |
|
The outcome of the local adverse event review had been shared with the key individuals involved for reflection and learning to include improvement in documentation. Teaching sessions were in progress, commencing in July 2022. |
By: 21 February 2024 |
The Adviser noted that the policy for the management of superficial vein thrombophlebitis does not include information about the monitoring of blood results which should be done for patients being treated with heparin. If this information is included in a separate policy, it is suggested that consideration is given to including a link or reference to the relevant policy that gives such detail, or to include the detail in the SVT policy itself.
In this month’s edition of the Ombudsman’s findings, we highlight the importance of taking good notes during a complaints investigation and using these to help communicate openly with the complainant.
At the 2023 SPSO Conference, Carolyn Hirst, Independent Consultant and Researcher at Hirstworks, delivered a fantastic session to delegates drawing on her own experiences and learnings to do with complaint handler wellbeing.
This month the Ombudsman’s findings highlight the importance of taking a person-centred approach.